
Two kinds of NHS reform
The Darzi report ends on a cliffhanger, and never quite tells us what the government's vision for NHS reform is

You wait ages for a big report on the Health Service, then two come along at once.
Yesterday we got not just the Darzi review of the NHS - but also a big chunk of the OBR’s annual Fiscal Risks Report was devoted to health.
Overall, the Darzi report has a lot more to say about the problems in the NHS than it does about the solutions.
It’s biggest idea is: the NHS needs a lot more money, particularly for capital.
Beyond that - while there are many good points made in it - it’s a frustrating document, because ultimately it doesn’t ever tell us what the government’s plans for NHS reform should be.
The OBR
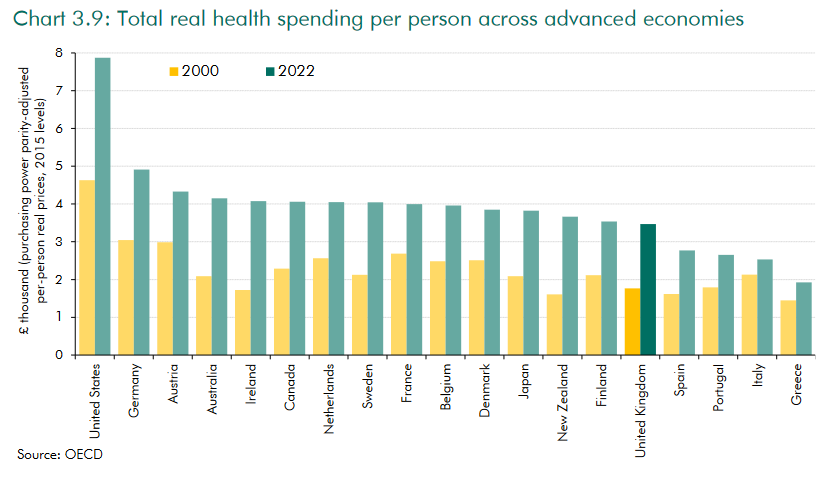
The OBR report provides really helpful context for all this. It shows that compared to other countries the UK is now somewhere in the middle of the pack in terms of the share of GDP spent on health, and has increased health spending relative to GDP by more than most countries over the last couple of decades:

But it also shows that lower GDP per capita means that spending per person isn’t that high compared to many places (noting that comparing GDP per person is always a bit subjective and relies on estimating PPP).
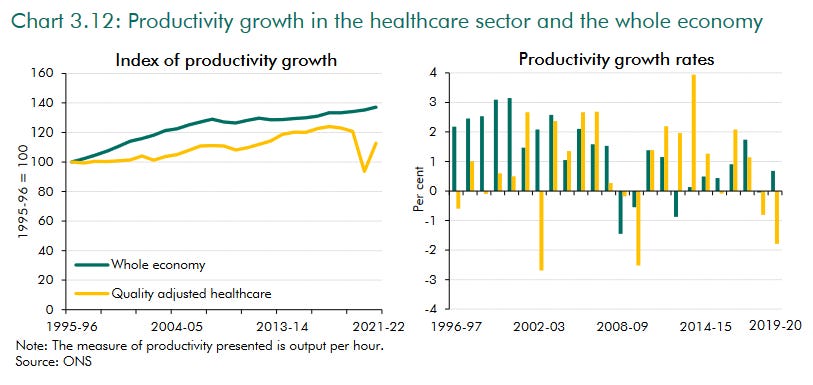
The OBR report shows how productivity in health has lagged the rest of the economy. And concerningly, in recent decades productivity growth has tended to be a mirror image of spending growth.
The Blair and Brown governments grew spending very rapidly. But average productivity growth, (even after adjusting for rising quality) was 0.7% a year from 1997/8 to 2009/10, less than half the rate (1.5%) of the period 2010/11 to 2018/19 when spending growth was slower:
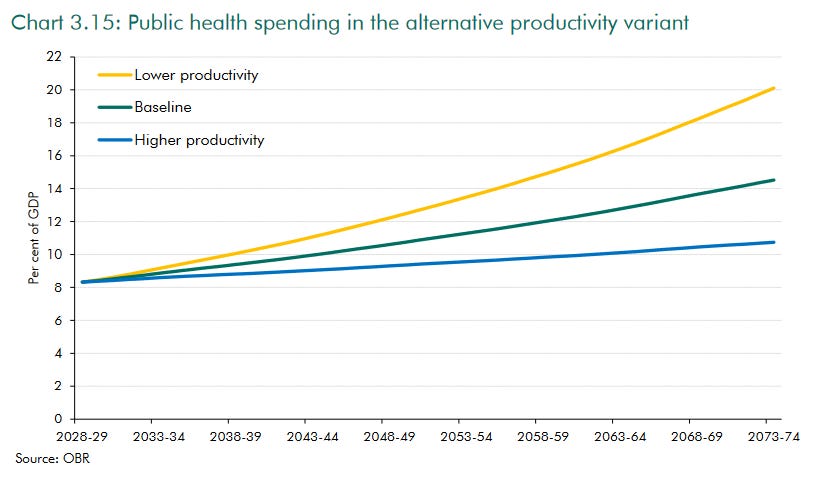
As I’ve written about before, have an ageing society which is likely to put upwards pressure on spending. Healthcare is a people business, so afflicted by Baumol’s cost disease. For these reasons the OBR expect health spending to grow - not just in real terms, but also as a share of GDP. That said, alternative assumptions about changes in health productivity growth could make the growth in costs much smaller or bigger. The resources freed up by a more productive health system could be huge:
So, to recap, although it was comparatively low in the past, spending in the UK now is neither crazy high or crazy low. Productivity growth has been slower than the rest of the economy and, rather than being faster when we grew spending faster, it has if anything has been slower when spending has grown faster. The growth of productivity has massive implications for our health but how much of our national income it will consume in future.
More money?
Darzi’s big idea is more money, and it’s pretty clear that people would like to spend more money on the NHS. In June, Ipsos found 61% of people were willing to accept personally paying higher taxes if it meant more money being put into the health service. Only 40% said the same about other public services or defence.
This is one of the main reasons Labour have been elected. While people do mainly think money is wasted in the NHS and many people think the structures and incentives of the NHS are wrong, many still want to spend more on it. Reform and more money has long been the position of voters.
For the Conservatives, now in opposition, we need to face up to a few things. People did accept, up to a point, that the problems in the NHS had been caused by the pandemic. But we will obviously not convince people that we are serious or have changed if we try to pretend everything in the NHS was rosy. It obviously isn’t.
For the Conservatives, any plans we come up with for reform will be much more positively received if we are also able to say at the same time that we will find more money. This is one reason I have previously argued that we should move money from elsewhere (say the aid budget) into health, and focus that extra health spending on the things that can raise productivity and prevent ill health. Something like a “productivity and prevention fund.” (But with a better name - I am not good at branding).
On the Conservative side we have a massive rebuilding task after our record defeat. It is true that Starmer is no Blair, and that Labour won on a small share of the vote (with three million fewer votes than Corbyn!) because of Reform splitting the right. And it’s true, they have got off to a very bad start.
But we also have to change - and decisively. One of the most important and difficult elements of that is getting our tone and policy right on health. We cannot look anti-NHS or come up with ideas people think are risky or wonky, and we must absorb the fact that health is something people DO currently want to spend more on.
Two types of reform
Many politicians talk about ‘reforming’ the NHS. I think there are two types of reforms.
There’s a first type of reform which you could call reform within the current structures - around which there is a reasonable degree of consensus, and which many politicians have advocated various aspects of. Type one reforms tend to be trying to attack a problem directly, often through central direction.
Then there are more fundamental types of changes you could call proper structural changes. I don’t mean changes to move to a totally different system like a European social insurance system - but things which change the operating logic of the NHS. Type two reforms attempt to address the underlying causes of underperformance, and to create a self-improving system, rather than relying on encouragement from the centre.
Both are important, but there tends to be less agreement about type two reforms.
To get specific, type one reforms are things like:
Spurring the uptake of technology
Improving transparency and performance data
Process improvements
Better workforce planning
Encouraging new modes of delivery
In type two are a set of different but related different reforms which have been tried over the years. People sometimes talk about ‘market reforms’ as a shorthand, but I’m not sure that is a good description for all of these things. They are really about creating a self-improving system. Examples include:
Fundholding. Giving GPs a larger part of the budget, so they can overcome the gravitational pull and imbalance of power that sucks all the money into (more expensive) hospital treatment. By making GPs purchasers they have incentives to control costs and drive performance in secondary care. GPs are the one ‘European-style’ part of the NHS, not owned by government, and are also the most popular bit. Fundholding was one of the big ideas of the 1991 reforms and has since been reinvented multiple times under different names: PCTs and “Practice Based Commissioning” in 2005, then again as “Primary Care Home” in the 2010s. There was pretty positive evidence that Fundholding made a positive difference - health policy academic Julian Le Grand (later an advisor to Tony Blair) noted that “the GP fundholders had shorter waiting times, reduced hospital referrals, reduced prescription costs”. Blair regretted letting Frank Dobson get rid of it in 1998.
Autonomy. The internal market of the early 1990s and the creation of Foundation Hospitals in the Blair era both reflected an attempt to change the incentives facing hospital managers. Instead of having the proceeds of local productivity improvements simply sucked away to fill holes elsewhere, managers would be able to retain gains locally, both rewarding and enabling reform at the local level. “Earned autonomy” was a 2000s version in which such autonomy was granted conditional of good performance, to both reward and spur better performance.
Choice. This was a key part of the Major-era internal market, and also a key part of the Blair-era reforms. Everyone would be able to choose and book the provider of their choice, the best providers would grow and patients could shift their treatment towards where there was more capacity and get treated faster. This was underpinned by payment by results - centres that did more got more money, rather than just a block payment. This system survived for a long time, it though collapsed during the pandemic and is has been in the process of being reestablished since.
Protection from capital rationing. A problem that affects all government-owned services is the short termism of elected politicians, leading to underinvestment in capital. In their initial conception Foundation Trusts were going to be able to borrow freely on the open market so that they could escape from Treasury capital rationing. But the Treasury were not so keen, and imposed borrowing limits.
Centrally-led reform
A classic type one approach to reform would be for ministers to get the system to make a list of how different organisations are performing on some metric, and then to try and enforce better performance. You could do this by having a checklist of things all providers have to do regarding that issue, or by putting the bottom performers into special measures and making them come up with action plans and the like.
Or you can change processes. For example, the last government was pressing local authority and NHS social care planners to co-locate, which improves communication and patient care.
There is a lot that can be done simply by getting the system to address the massive variations in performance between centres with similar patients and similar resources. Darzi’s report features some striking examples of massive and unjustified variations in performance. Take long waits in A&E. Shropshire and Somerset are both quite rural, but one is doing well, and the other badly. Merseyside and South Yorkshire are both quite urban. One is doing much better than the other:

There are endless examples like this in the NHS. One example, which Labour are less keen to highlight, is the massive gap between Wales and England in terms of long waits. If this was only about an older population in Wales we would see the same in the North East of England, but we don’t.
When it comes to centrally-led improvement, I think the big thing we need to do more of is to sack or manage out weak mangers.
Good managers can make a massive difference to the lives of people across a wide area. And when you see the massive differences in performance across different parts of the NHS and between very similar areas it is so clear that it isn't just about money. But at present there is too little accountability for those who are not performing. In other industries it is normal for the bottom performers to be managed out each year and that is something the NHS could learn from. Staff are the first to suffer when management is poor, and many of the great people in the NHS are demoralised when they have to carry managers who are no good.
Underperforming managers do sometimes leave in the NHS, but not often enough.
But centrally-led improvement is not the whole answer. The National Programme for IT is probably the most infamous example of a centrally-driven programme abjectly failing, because of a lack of buy-in locally, and a lack of gradualism.
Another example: all hospital trusts are supposed to have Electronic Patient Records by spring 2026. NHSE can try to centrally enforce that deadline. But wait a minute - how come GPs all had equivalent technology by the 1990s? Why have their incentives and ability to execute this been so different to the hospital trusts? (Hint: they were free to invest their own money and reaped the benefits directly).
More generally, why do positive innovations spread so slowly in the NHS? Asking those questions takes you towards type two reforms.
There is a role for central management, but if you can change incentives and allow the best centres to do more, the results can be so powerful. During Rishi Sunak’s time as PM the system of payment by results was turned back on for elective care, and as Darzi notes, performance there has been better than in Emergency care, which remains on block payments since the pandemic.
My experience and the last government
A lot of the type one reforms that Darzi does touch on were also on the agenda of previous Conservative Secretaries of State. In my own brief when I was Minister for Primary Care we did all these sorts of things. We funded the rollout of new cloud-based phones to GPs, which means you should never get an engaged tone, and allows people to request a call back rather than hanging on the phone. Some GPs use this, others do not. We funded GPs to get them new tools to accept and triage requests from patients online. Some are really making the most of this to improve access, but not all.
We started to publish new data on the outputs of GPs and dentists on fingertips and met with ICBs that were doing badly to chase them to up their game - meetings NHSE disapproved of. We agreed a detailed plan to hack back some of the bureaucracy at the interface of primary and secondary care which eats up time for doctors and patients - though NHSE then hated being asked to measure and enforce progress on this.
We introduced a new service - Pharmacy First - which lets people get treatment for common conditions at the pharmacy, so taking the pressure off GPs.
I was responsible for public health and in that field we also pushed quite a lot of new modes of delivery: sending out home tests for HIV; sending a million smokers vapes to encourage them to ‘swap to stop’; experimenting with tech and whole-city efforts to encourage physical activity in Wolverhampton and rolling out a new service that takes eyecare services direct to pupils in special schools.
Similar things were happening in other bits of the service: in elective care, emergency care, social care, community care and so on.
And some bigger things were happening too. For the first time since its creation the 2023 Long Term Workforce Plan actually sets out a clear plan and timescale to grow each element of the workforce. This is a genuinely massive change which Darzi is a bit quiet on, but will require serious commitment to deliver.
There’s masses more to do on all these fronts. While there are not million pound notes lying on the ground, there are opportunities to do things better by directly instructing the system to do things.
But but but… the experience of trying to make some of these things happen from the centre is often like wading through treacle.
There are two possible responses to this - which could be in tension, but you could try and do a bit of both of.
First, you could ramp up the ability of the centre to push through type one reforms, and improve your ability to wade through the treacle.
Or you could try and get some type two reforms going so that you have to do less from the centre. Or indeed, you could try ramp up both.
But it’s not 100% clear what Darzi thinks about either of these possibilities.
Darzi
As you would expect, Darzi spends a lot of his report making the case for more money: specifically for higher rates of capital spending, in order to get more productivity-enhancing technology into the NHS.
He says that “there is a shortfall of £37 billion of capital investment”. Given HMT have allowed the inclusion of this figure in the report, I assume Rachel Reeves will be announcing a package which tops up the capital budget by at least that amount over the next few years.
But beyond more money for capital1, what is the big vision? Is it a vision of centrally-led improvement, or a Milburnian one, of self-improvement through competition, choice and earned autonomy? Or both?
When it comes to the ability to lead reforms from the centre, Darzi is critical of the 2012 reforms. So am I, though perhaps for slightly different reasons.
He talks twice about the reforms “dissolving the NHS management line”. He thinks the 2012 reforms were too big and too chaotic, with too many new organisations created and changed; that the CCGs were sub-scale and that the new ICBs are better. He also seems to argue that there are too many regulators, too many central bodies and that the centre is probably too big.
I agree with quite a lot of that, and as Health Secretary Steve Barclay was shrinking the centre quite determinedly to free up resources for the frontline.
But I would add something else: we have ended up in a system where NHSE is highly autonomous of ministers, but doesn’t like doing the performance management of local systems. This is a legacy of the idea of “independence for the NHS” in the 2012 reforms.
In particular, the separation of the finance function of NHSE from DHSC cuts off ministers from access to the information they need about how many is being spent. The NHS is actually run on a day-to-day basis not from the Department of Health, but from NHSE HQ at Wellington House.
Sure, the process of increasing autonomy from ministers which began under Kenneth Clark was probably sensible up to a point - but it has gone too far.
But will the current government unwind it? It is not clear from Darzi what the plan is for central leadership.
A self-improving system?
I thought the most interesting parts of the Darzi report are those which talk about the need to get the forces of self-improvement in motion. As he notes in the intro:
“The NHS in England has emulated Wales and Scotland and changed its improvement philosophy from competition to collaboration. The framework of national standards, financial incentives and earned autonomy as part of a mutually reinforcing approach is no longer as effective as it once was, and needs to be reinvigorated.”
Later on, at page 127 he makes some fairly clear criticisms of the shift away from type two reforms in the middle of the last decade (my bold).
“Over the past decade, there has been a significant shift in payments away from activity-based mechanisms, although they remain in place for elective care. By doing so, funds have become more consolidated and less transparent. National pricing has been replaced with block contracts where providers are funded for their efforts rather than their outputs. It is perhaps not a coincidence that the drop in clinical productivity metrics for the urgent and emergency pathway is nearly double that for outpatients and elective surgery, since it remains on block contracts.”
He notes that the Treasury’s desire to control costs has eroded away freedoms in the system:
As the number of organisations in deficit has risen, the amount of funds held centrally has increased in order to balance the system as a whole. While there can be no doubt about the expediency of this approach, over the longer-term it risks complacency in providers who may begin to believe they will always be bailed out.
At the institutional level, trusts no longer advance to foundation trust status, since a policy decision was taken to cease the foundation trust pipeline in 2016, and the status itself has been diminished as they have lost their freedom to determine capital spending. This was imposed in response to the overall capital constraints set by HM Treasury but reduces the incentives for Boards to develop their organisations. It drives intense frustration when organisations have the cash available to fund investment but are not permitted to spend it.
Read on a bit further and it sounds like the report is just about to advocate a big shift back to type two reforms:
Since the 1980s and the creation of the internal market, the NHS has used quasi- markets to promote efficiency improvements. In acute hospital services, this saw funding shift from being based on inputs to being linked to activity and ultimately to following patients according to their choices. The idea was that this would create competition in the market for elective services which would encourage providers to reduce waiting times and improve patient experience. This was part of the way in which the NHS got to peak performance during the first decade of this century.
Under the NHS Constitution, patients continue to have the right to choose their provider. But in practice, patients are not routinely asked where they would like to receive their care; to exercise their rights, they must demand them of their own volition, and nearly half of adults are unaware that they have a legal right to choose. The practical effect has been that the quasi-market for elective care services has been weakened. This is despite the fact that choice remains popular, with 75 per cent of the public agreeing that they should have a right to choose their provider, in opinion polls.
But but but… just when you think the choice agenda is back, the report just ends rather abruptly, and in a very ambiguous way.
“Yet despite all-but eliminating the role of markets, the NHS is yet to fully embrace the planned alternative. The NHS Long Term Plan was published in 2019, but was quickly superseded by events with the outbreak of the pandemic the following year Since then, political demands have pushed the NHS to a short-term operational focus and the priority has been to recover performance.”
I turned the page to find the punchline, but there isn’t one.
So… is the answer the “planned alternative”? Or to bring back quasi markets? If so how and why and when? Will emergency care go back onto payment by results? Will GPs get to be fundholders again? Will Foundation status be revived, with fiscal autonomy and freedom to borrow? It’s not clear.
To get the forces for self-improvement going will require a clearer vision and a lot of pushing. Because for various reasons many actors in the system don’t like type two reforms. Managers in secondary care rather like a guaranteed income, rather than being subject to the risks of patient choice. There are plenty of mechanisms for them to hobble the choice agenda locally. They certainly don’t want their budgets handed over to GPs. The Treasury has historically blown hot and cold about the choice agenda at best. The institutional Treasury generally sees these reforms as risky and uncertain, and doesn’t like the idea of local borrowing or even retained surpluses.
Conclusion
I assume that DHSC will get quite a big wodge of cash in the forthcoming budget. Waiting lists should also continue to fall post pandemic. Things will get better. The question is will they get enough better.
As well as investing the money in productivity-enhancing technologies, its arrival should be the opportunity to set up some self-improving dynamics.
The big thing the NHS needs to do, is to get better at caring for older people with multiple health issues in the community, rather than sucking them into expensive hospital care. It is frightening how quickly older people can deteriorate if they get stuck in a hospital bed, even for a day or two.
Getting there is partly about building up primary care capacity, but also about giving GPs the power within the system to move services out of hospital and into the community. Then joining up frail elderly care in general practice with social care.
Darzi is right that the last couple of years have been about getting the system back on its feet post pandemic. The next couple of years need to be about getting self-improvement and productivity moving, and reconfiguring the NHS for an ageing society.
He does say a bit about public health, which I will come back to another time.
"Darzi’s big idea is more money, and it’s pretty clear that people would like to spend more money on the NHS. In June, Ipsos found 61% of people were willing to accept personally paying higher taxes if it meant more money being put into the health service. Only 40% said the same about other public services or defence."
Did you see the polling that Dan Neidle did on this? When asked more specifically on how MUCH more in taxes people were willing to spend, the average amount (I believe, the mean) extra, that people were willing to pay, was a paltry £10.
So I think it's important that one discerns between virtue signalling (on which, let's face it, this is an example), and the sacrifices that taxpayers would be willing to make in practice!
In fairness to Lord Darzi (disclosure: I’ve known Ara for nearly 20 years and I’m a big fan), he wasn’t asked to make sweeping recommendations for reform (which supposedly will come in the government’s 10-year plan) but simply to diagnose the problems and “start a conversation”.
https://www.gov.uk/government/publications/independent-investigation-of-nhs-performance-terms-of-reference/independent-investigation-of-nhs-performance-terms-of-reference
But in general I agree with almost everything you say. Alan Milburn (for my money the best secretary of state of the last 30 years) got a hell of a lot right and his emphasis on choice, outcomes and autonomy was the way the NHS has to evolve in order to improve.