
What we need from the Dentistry plan

For some time DHSC has been working on a plan to fix NHS dentistry. I worked on it as a minister.
Here are the top three things we need from it.
1) Funding to get dentists taking on new patients again
The most pressing challenge is to get dentists to take on new NHS patients. Large rural areas of England don’t have any dentists taking on new adult NHS patients (black dots below), and the people without a current connection to a dentist struggle the most to get treatment. You can explore the map below at nhsdentists.bathdata.org

Greater Manchester NHS pioneered a 'new patient bonus' last spring – about half of NHS dentists took it up and by last summer GM dentists were four times more likely to be taking on new patients than the national average - that's one reason the map above looks the way it does. So a national bonus could make a big difference.
2) A move over time to rational funding formula
Uniquely among NHS services, NHS dentistry has never had a funding formula. Until 2006 spending was essentially demand-driven. Since then, places essentially just get whatever they got in 2006, even if they have many more old people and so much higher need.
This is leading to massive variations in the proportion of commissioned Units of Dental Activity which can actually be delivered. Urban areas are somewhat better off, while shire areas are losing out. Dentistry needs to move to a funding formula.
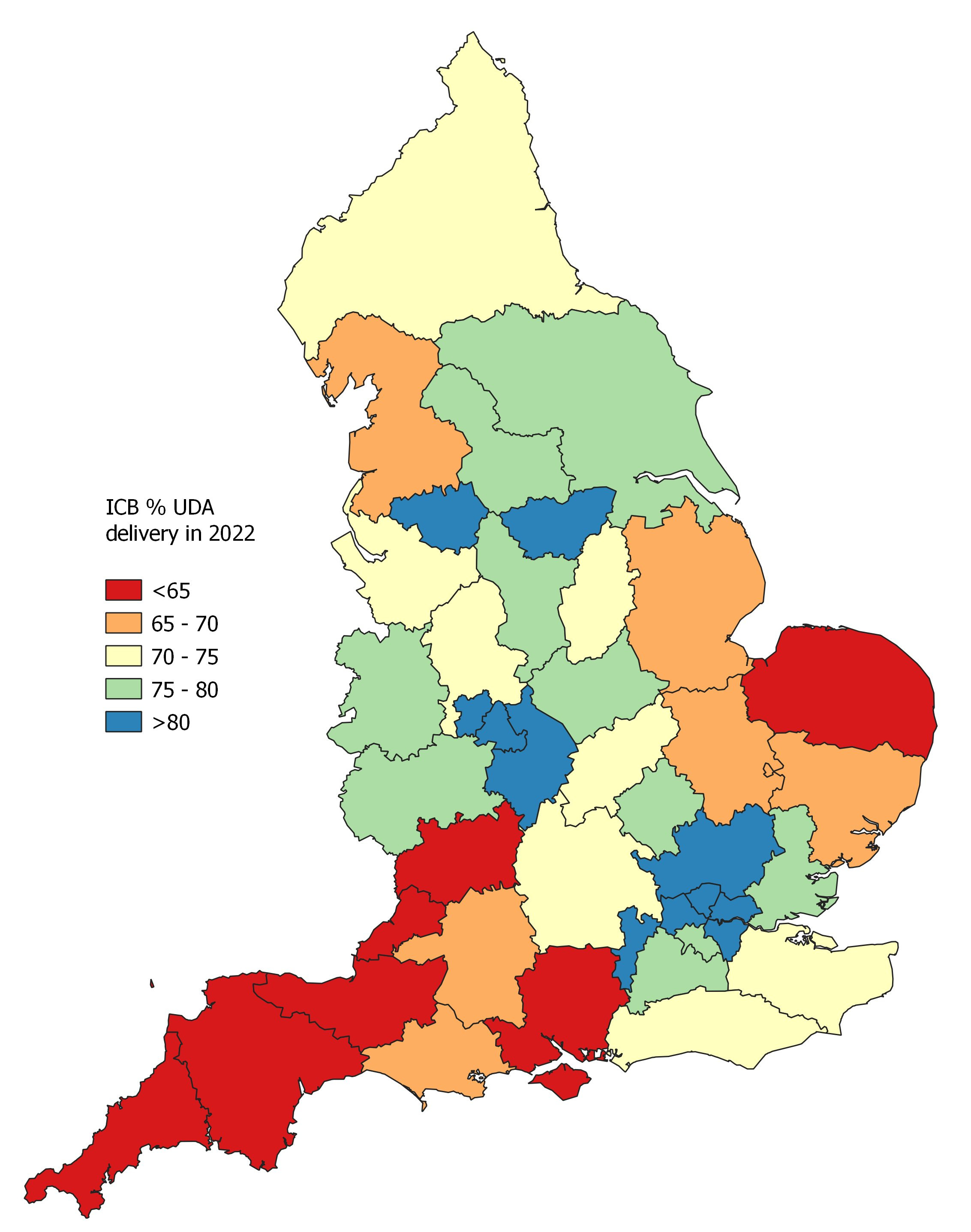
There was always some variation in delivery. Since the pandemic it has massively increased. Though activity is shaply recovering, data from Fingertips shows how performance between ICBs has fanned out, with shire areas much slower to recover than urban.
In 2018 UDA delivery between ICBs varied between the high 80s and nearly 100%. Now the variation is much greater, with rural areas slowest to recover.
3) An overhaul of the broken 2006 contract
The contract put in place by Labour in 2006 needs a massive overhaul. The 2006 contract reflected Treasury concerns about cost control & incentives to over-treat. We went from hundreds of payments, matched to the cost of work, to just three broad bands with spending capped.
The problem is that one size doesn’t fit all, and too many treatments cost dentists more to deliver than they get paid. The government has recently started to split bands which has had a positive effect. But we need to go further.
In particular, some complex patients with poor oral health need way more work than can be accommodated by the current contract system. For starters, they need carving out, with something more like the simple, capitated payments that GPs receive.
The variation in how much individual dentists are paid is unjust and also a disincentive to keep doing NHS work. Two dentists on one street can be paid totally different amounts for doing the same work.
he effective UDA rates reflect the patient & treatment mix that practice had in 2005 & were sprung on dentists. Over time rates are becoming less and less anchored to any reality. Where funding and UDA rates are lower, delivery is genrally lower - the below is 2021/22 data.

You can see it on a map too. Blue dots = high payment rates, Darker areas = higher delivery rates Red dots = low rates Lighter areas = lower delivery rates
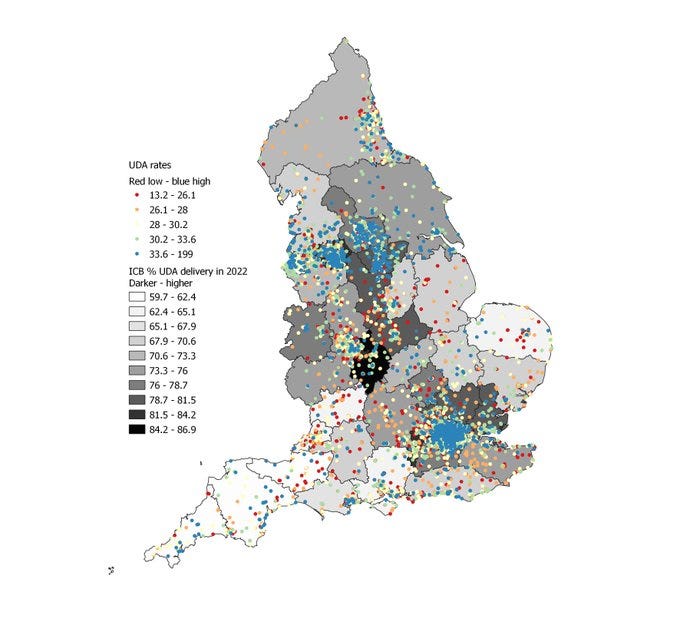
The minimum UDA rate recently introduced by the government helps, but needs to go further. Dentists on lower rates may obviously be more likely to stop or reduce NHS work. Though some effectively renegotiate, others stop or do less NHS work.
Progress is being made: The amount of NHS dental activity delivered has gone up nearly a quarter over the last year. Dentistry training places will increase by 40% under the long term workforce plan, which will really help in the long term.
But we need to get a properly funded dental recovery plan out ASAP. Dentists are private and will treat NHS patients if the price is right. At present only a small number are taking on new NHS patients. We can see they respond quickly to incentives. We can & must fix this!
Neil, the Conservative Party in its 2010 manifesto said that a new plan for Dentistry would be brought in ungently as the 4 year old plan was not working, 14 years later you are saying the same thing again as nothing other than reducing the funding as been done so far.
As the last governments plan has been in place for 18 years of which 14 were under this government you must have after all been at least thought it could continue and didn’t need to change or else why has nothing changed ?
Could you enlighten your constituency's electorate by saying why the government hasn’t carried out the 14 year old promise? Also what will it now cost to return this service to what it was 14 years ago or even to improve it to an acceptable standard ? and where is that money coming from as we are continually being told there is no money ?
Thank you.
May be a mark of privilege, but I didn't realise you could get NHS dentistry until a was a teenager, and have never used it.
Still not clear to me why it exists. An annual private hygienists vist costs ~£70 – just over half the cost of a Netflix subscription – and the price is half that for kids.
In other words: anyone can afford it.
I'm sure there are more
productive uses of £3bn taxpayer money. Perhaps it's best to continue the effective budget freeze and let inflation kill it off?